
Osteoarthritis vs Rheumatoid Arthritis Differences: What Actually Matters for Your Joints (and Your Daily Life)
If you’ve ever sat across from a doctor, hoping for a straight answer about those aching knees—or watched a loved one struggle with morning stiffness so relentless it steals an hour of their day—you know the label matters. Not just for insurance forms, but for real life.

Here’s Where It Gets Real: They May Look Alike, But OA and RA Are Worlds Apart
Years ago, my own mother-in-law called me in a panic. She’d just had her second cortisone shot, but her knuckles were still red and puffy—and the pharmacist had mentioned “arthritis” without specifics. “But which arthritis?” she asked.
It’s not just her. Every week, I get emails from readers confused about the differences between osteoarthritis (OA) and rheumatoid arthritis (RA). If you’re nodding along, trust me, you’re not alone.
Here’s the kicker: OA and RA might both target your joints, but the way they do it—and what that means for your lifestyle—couldn’t be more different.
A (Quick but Crucial) Crash Course: What Is Osteoarthritis?
OA is the classic—what your grandparents likely called just “arthritis.” If you peek inside a knee with OA, what you’ll see is thinning cartilage, a bit like worn-down tread on a tire. Over time, the cushioning fades, and bone rubs on bone. Ouch.
What causes that? Mostly wear and tear. Age, repetitive motion jobs (think: nurses, mechanics, athletes), history of joint injuries—these are the usual suspects. According to the Arthritis Foundation, OA affects over 32 million Americans, and knees are the most commonly hit joint. Hip, hand, and spine OA are close behind.
I’ve seen folks get OA in their forties, but it’s far more common after 50—and especially in women after menopause, thanks to hormonal shifts.
So, What About Rheumatoid Arthritis?
RA is a whole different beast. Imagine your immune system as an overzealous security guard. In RA, it just can’t distinguish between friends and foes—so it starts attacking your joint lining (the synovium). The result? Inflammation, swelling, and pain that’s often symmetrical—both wrists, both knees, both hands.
And here’s the thing: RA is less common than OA (about 1.3 million Americans, per the CDC), but it can strike young adults—sometimes as early as their twenties or thirties. Women, again, are at higher risk. It’s an autoimmune process, and although genetics play a role, the triggers are still a bit of a medical mystery.
Symptoms: How Can You Tell Them Apart?
Let’s get practical. Here’s what you should actually look for (from years of watching patients walk into my clinic with both):
- Morning stiffness? Both can cause it, but in OA, it usually eases within 30 minutes; RA stiffness can last an hour or more, sometimes half the morning.
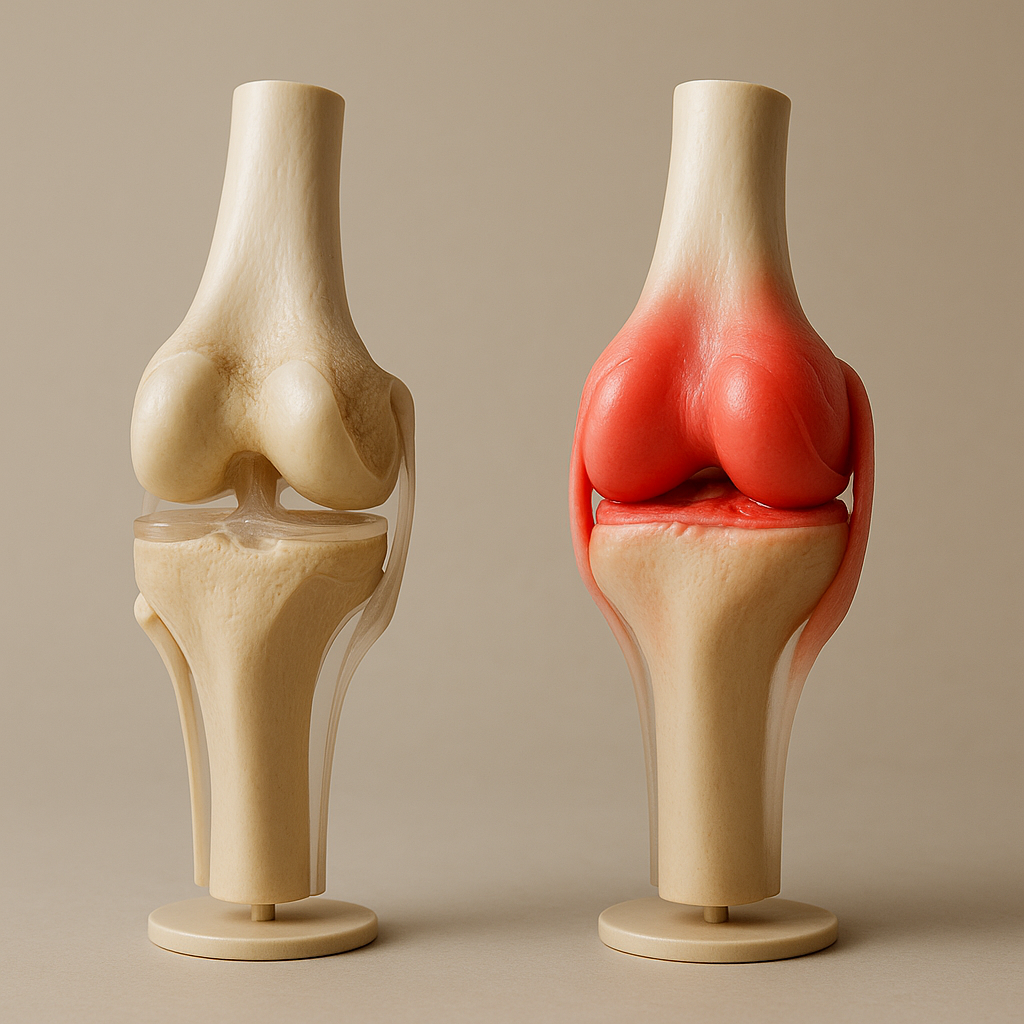
- Swelling? OA can cause mild swelling, but RA’s inflammatory storms can balloon joints visibly—and with heat and redness.
- Which joints? OA loves weight-bearing joints (knees, hips), plus the tips of fingers (DIP joints). RA prefers smaller joints—wrists, knuckles, base of fingers (MCP, PIP), often in pairs.
- Systemic symptoms? This is the game-changer: RA can bring fatigue, fever, even weight loss. OA almost never does—it's a local joint issue.
Look, I know checklists can’t replace a doctor’s visit. Bloodwork (rheumatoid factor, anti-CCP antibodies) and imaging matter—a lot. But if those symptoms made you raise your eyebrows, jot them down and take them to your next appointment.
The Science (Without the Medical Jargon)
I promised you details, so here goes. OA is fundamentally a degenerative joint disease. Cartilage wears down, bones may develop little spurs (osteophytes), and sometimes the body tries to patch things up by laying down extra bone. No surprise, that hurts.
RA, on the other hand, is a systemic autoimmune disorder. The immune system ignites a fire inside the synovium, the sensitive lining of your joints. Over time, that inflammation erodes cartilage and bone. In severe cases, it can also affect organs—lungs, heart, even eyes.
Here’s a jaw-dropping stat I always mention: One 2014 BMJ study found that untreated RA can shorten lifespan by as much as 10 years due to systemic inflammation. That’s why it’s not just “joint pain”—it’s a whole-body condition.
Comparing Causes: Not All Arthritis Is Created Equal
- OA: Age, previous injury, obesity, overuse, genetics
- RA: Genetics, smoking history, certain infections, immune system malfunctions
Most articles gloss over this, but being overweight is a much bigger risk factor for OA than for RA. Each pound of extra weight adds about 4 pounds of pressure on your knees (per Arthritis & Rheumatology, 2015). That’s why weight loss—even just 10 pounds—can make a real difference for OA folks. For RA, weight is less important than controlling autoimmune triggers.
Diagnosis: How the Pros Separate OA from RA
I’ll be honest—sometimes even the best rheumatologists need a combo of tests and follow-up visits to be sure. Here’s what usually happens in a real-world clinic:
- Imaging (X-ray, MRI): OA shows joint space narrowing, bone spurs. In RA, early on, imaging may show swelling (effusion), then erosions in the bone near the joint.
- Blood Tests: RA can trigger positive rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies. OA? These are usually negative.
- Physical Exam: Doctors look for pattern—symmetry, warmth, nodules, deformities. Swelling at the tip of your fingers? That’s probably OA. Puffy knuckles with morning fatigue? More likely RA.
Health disclaimer: Don’t self-diagnose—make sure you talk to your healthcare provider for bloodwork and imaging, especially if you have new or worsening symptoms.
Treatment: What Actually Helps (and What Doesn’t)
Now for the meat and potatoes. Treatment plans aren’t one-size-fits-all—what works for OA could be useless or even counterproductive for RA, and vice versa.
For Osteoarthritis:
- Exercise & Strengthening: Good news: you don’t have to run marathons. Gentle range-of-motion and low-impact strength work (like what you’ll find in Treat Your Own Knees) can boost joint stability and reduce pain. I’ve sent dozens of clients home with those basic routines—more often than not, they come back surprised by the improvement.
- Weight Management: This isn’t about aesthetics—it’s about physics. Drop 10 pounds, relieve up to 40 pounds of pressure on your knees (the math doesn’t lie).
- Over-the-counter topicals: For fast relief, things like Voltaren Arthritis Pain Gel (diclofenac) are now FDA-approved and can genuinely help with mild-to-moderate OA pain. I use this in-clinic all the time—patients like that it’s not greasy and doesn’t have the “medicine smell.”
- Mobility aids: Braces, canes, orthotics—these are tools, not signs of defeat. A knee brace like the NEENCA Professional Knee Brace is a smart pick for those who need extra support but want to stay active. The side stabilizers make a noticeable difference for unstable joints.
For Rheumatoid Arthritis:
- Early and aggressive medication: The gold standard is a DMARD (disease-modifying antirheumatic drug) like methotrexate, sometimes paired with a biologic. Don’t wait—the earlier you start, the more joint function you keep.
- Physical therapy: Gentle movement is still key, but you’ll likely need a personalized plan. I tell my RA patients: “Move as much as you can on good days, but honor your limits when fatigue strikes.”
- Pain relief: Topicals and braces can help some, but RA pain often needs systemic treatment. NSAIDs or corticosteroids may be used during flares, but they’re not long-term fixes.
Here’s the controversial bit: While supplements (like glucosamine or turmeric) get a lot of press, the Journal of Rheumatology 2020 meta-analysis found only modest benefits for OA—and almost zero for RA. Save your money for proven treatments.
Living With Each Type: What’s Life Really Like?
I’ve watched clients with OA limp into my office, frustrated that stairs have become the enemy. But with the right home exercise plan and a brace, I’ve seen folks return to hiking, gardening, even ballroom dancing. OA symptoms tend to be mechanical—worse with movement, better at rest.
RA, meanwhile, is unpredictable. Flares can hit out of nowhere—one reader even told me hers showed up after a stressful week at work. But here’s some hope: with today’s meds, a lot of RA patients are in remission or have only mild symptoms. It’s not a life sentence of pain.
Impact Beyond the Joints
RA can affect energy, sleep, mood, and even heart health. (One 2019 Arthritis Research & Therapy paper found that RA raises your risk for cardiovascular disease by about 1.5 times.) OA, on the other hand, mostly impacts mobility and quality of life—but doesn’t carry the same systemic risks.

Frequently Asked Questions: Quick Answers from the Clinic
- Can OA turn into RA? No—these are separate conditions. But, rare people can have both.
- Is one more “serious” than the other? Both can be disabling, but untreated RA poses larger long-term health risks due to systemic inflammation.
- Which is more painful? Depends on the person and the flare, but RA pain is often more severe and unpredictable.
- Are there blood tests for OA? Not really—OA is diagnosed mostly by symptoms and imaging. RA requires blood testing for confirmation.
- Does diet make a difference? For OA, weight loss helps; for RA, some find anti-inflammatory diets useful, but meds are still primary.
Takeaways You Can Actually Use
- Know your diagnosis. OA and RA are not interchangeable—accurate diagnosis means better-targeted care.
- Movement is medicine. Period. Whether it’s gentle stretching, strengthening, or even aquatic therapy, movement trumps rest for both types (with adjustments for flares).
- Support matters. Don’t be shy about braces, topical medications, or guided home programs like Treat Your Own Knees—they aren’t magic, but the right tools make a difference.
- See your provider. If your joints swell, you have fevers, or “arthritis” is suddenly everywhere, get a workup. Early action changes outcomes—especially for RA.
The Bottom Line: It’s Not Just Semantics
I know “osteoarthritis vs rheumatoid arthritis differences” might sound like textbook jargon, but I’ve seen the real-world impact of getting it right. The right diagnosis can mean the difference between endless frustration and feeling like you’ve finally got a handle on your health.
If you’re in doubt, write down your symptoms, try some gentle movement, and (please!) have an honest chat with your doctor. Need a jumpstart? I’ve found resources like Treat Your Own Knees and smart tools like the NEENCA Professional Knee Brace can be game-changers for OA, while topical relief like Voltaren Arthritis Pain Gel is a practical addition for both.
And if you have a story to share—what’s worked for your joint pain, or which diagnosis tripped you up—drop me a line. I read every single message.
Stay moving, stay curious, and don’t let a diagnosis define what you can do.
James Chen, MS, CSCS
Exercise Science, Certified Strength & Conditioning Specialist
JointReliefReviews.com columnist